🎧 Busy Parent? Listen to the Quick Summary (5 mins)
Executive Summary: The Climatological and Entomological Convergence
The austral summer of 2025/2026 presents a uniquely complex and elevated risk profile for vector-borne diseases in Australia, driven by a converging set of high-impact climatological variables. The Bureau of Meteorology (BOM) and international climate models have confirmed that Australia is currently under the influence of a La Niña event in the tropical Pacific, coupled with a negative Indian Ocean Dipole (IOD) that, while weakening, has left a legacy of hydrological saturation across the continent.1 This climatological setup is historically associated with above-average rainfall, cooler daytime temperatures, and significantly increased humidity across the eastern and northern seaboards, creating a biosphere that is exceptionally conducive to mosquito proliferation.3
The significance of this weather pattern extends far beyond simple precipitation metrics. The Sea Surface Temperatures (SSTs) in the Australian region were recorded as the second warmest on record for October 2025, with warmer-than-average waters predicted to persist through February 2026.1 These elevated SSTs act as a thermodynamic engine, providing increased moisture and energy to the atmosphere, which enhances the severity of storm systems, cyclones, and rain depressions.4 For the Australian public, and specifically for parents of young children, this translates into a biological imperative: the management of mosquito-borne threats in an environment that heavily favors their reproduction.
The hydrological loading of inland river systems and the creation of ephemeral wetlands provide optimal breeding conditions for floodwater mosquitoes. Unlike container-breeding species that rely on urban water accumulation, floodwater mosquitoes lay eggs in dry soil that can remain dormant for years; the inundation associated with La Niña triggers massive, synchronized hatching events that can overwhelm local control measures.5 Entomological surveillance has already detected the consequences of these conditions. Japanese Encephalitis Virus (JEV) was detected in mosquitoes in the Horsham region of Victoria in late November 2025, a timeline significantly earlier than expected for the southern states.7 Furthermore, Ross River Virus (RRV) and Barmah Forest Virus (BFV) detections have been noted in South Australia and Western Australia, signaling a continent-wide activation of viral vectors.9
This report provides an exhaustive analysis of the risks posed by this specific La Niña summer, the physiological vulnerabilities of infants to mosquito bites and mosquito-borne diseases, and the scientific efficacy of natural protection strategies. It serves as a foundational guide for navigating the 2025/26 mosquito season with a focus on organic, non-toxic interventions suitable for the most sensitive demographic: babies and toddlers. It critically examines the Kidsbliss organic formulation against the backdrop of Australian regulatory standards, offering a scientifically robust roadmap for parents seeking to balance efficacy with safety.
Part I: The 2025/26 Vector Ecology and Environmental Drivers
1.1 The La Niña Multiplier Effect
The relationship between La Niña and mosquito population dynamics is non-linear and biologically potent. It is not merely a case of "more rain equals more mosquitoes"; rather, it is about the persistence and distribution of water in the landscape. La Niña conditions typically sustain water in the environment for longer periods, preventing the drying out of ephemeral pools and allowing for the completion of the mosquito life cycle—from egg to larva to pupa to adult—which can occur in as little as a week in the warmer temperatures associated with the current SST anomalies.11
During the extensive flooding events of the 2010–2012 La Niña years, Australia witnessed major outbreaks of mosquito-borne diseases, including Murray Valley Encephalitis (MVE) and virulent strains of West Nile Virus.6 The 2025/26 season mirrors these historical conditions but with the added variable of climate change intensifying the hydrological cycle. The Bureau of Meteorology’s long-range forecast indicates equal or above-average chances of rainfall for eastern Australia, but more critically, the existing soil moisture profiles mean that even average rainfall can result in significant surface water retention.4
The specific risk for the summer of 2025/26 is the "floodwater" mosquito. Genera such as Aedes and Culex are particularly adept at exploiting these temporary water bodies. As waters recede following the heavy rains predicted for December and January, they leave behind pools that are disconnected from flowing water. These pools are ecologically distinct because they lack predatory fish that would typically consume mosquito larvae, creating ideal, unchecked nurseries for massive population explosions.
1.2 Oceanographic Influences: The SST and IOD Factor
The driver of this biological risk is deeply rooted in oceanography. The Sea Surface Temperatures (SSTs) surrounding Australia are currently exceptionally high—the second warmest on record for October 2025.1 Warm oceans provide the latent heat energy required to fuel atmospheric instability. This increases the probability of tropical cyclones and deep low-pressure systems moving further south than usual, potentially bringing tropical mosquito species and the viruses they carry into temperate zones.
Simultaneously, the negative Indian Ocean Dipole (IOD), while weakening as summer progresses, has primed the continent with moisture.1 A negative IOD typically results in warmer waters near Western Australia and increased rainfall across southern Australia. The combination of a Pacific La Niña and a negative Indian Ocean Dipole is a rare "double driver" event that historically correlates with the most severe mosquito seasons on record. The persistence of warm waters off the east coast is expected to maintain high humidity levels well into autumn 2026, extending the mosquito season significantly beyond its usual peak.4
1.3 The "Floodwater" Phenomenon
The mechanism of the current threat lies in the reproductive biology of floodwater mosquitoes. Species such as Aedes vigilax (the saltmarsh mosquito) and Aedes vittiger (the grey striped mosquito) do not lay eggs on the surface of water like other species. Instead, they deposit eggs in moist soil or mud in areas prone to flooding. These eggs enter a state of diapause (dormancy) and can remain viable for years, withstanding drought and heat.
When the heavy rains associated with La Niña inundate these areas—whether they are inland river floodplains or coastal saltmarshes—the water acts as an environmental trigger. The drop in oxygen tension caused by the wetting of the eggs stimulates hatching. Because millions of eggs may have accumulated over several dry years, a single La Niña flood event can trigger a "super-hatch," resulting in clouds of mosquitoes emerging synchronously days later.6 This phenomenon makes control extremely difficult, as the breeding sites are vast, often inaccessible, and the population boom is sudden.
For parents, this means that even if they live kilometers away from a permanent water source, they may suddenly find their homes inundated with mosquitoes following a heavy rain event, as the adults can disperse widely in search of blood meals.
Part II: The 2025/26 Viral Threat Matrix
The health implications of this mosquito explosion are categorized not just by the nuisance of bites, but by the specific pathogens currently circulating within the vector population. Surveillance data from late 2025 indicates the active transmission of several key arboviruses, necessitating a heightened state of alert for families.
2.1 Japanese Encephalitis Virus (JEV): The Critical Threat
JEV represents the most severe threat to public health in the current season. Once confined to the far north and parts of Asia, JEV has established a reproductive foothold in the temperate south-east of Australia. A rare but potentially fatal disease, JEV causes inflammation of the brain (encephalitis).
The first detection of JEV in Victoria for the 2025/26 season occurred on December 1, 2025, in the Horsham Rural City Council area.8 This early detection is alarming as it precedes the peak summer heat, suggesting a prolonged transmission window. NSW Health has also issued warnings following detections in sentinel animals, indicating widespread viral activity across the Murray-Darling Basin.13
2.1.1 Transmission Dynamics and Reservoirs
JEV is maintained in a zoonotic cycle between mosquitoes (primarily Culex species) and amplifying hosts, specifically waterbirds (herons, egrets) and pigs. Humans are considered "dead-end hosts," meaning they can become infected and sick, but they do not develop sufficient viremia (virus levels in the blood) to infect feeding mosquitoes.14
The La Niña conditions enhance this cycle by creating expanded wetlands that bring waterbirds into closer proximity with human settlements and piggeries. The flooding allows waterbirds to breed prolifically, providing a vast population of naïve hosts for the virus to amplify in, before spilling over into the mosquito population that bites humans.
2.1.2 Clinical Presentation in Children
Most JEV infections are asymptomatic. However, approximately 1 in 250 cases develops severe clinical disease. The onset is typically rapid and characterized by:
-
High fever and chills.
-
Severe headache.
-
Neck stiffness.
-
Disorientation, tremors, and convulsions (seizures), which are particularly common in children.
-
Progression to coma and potential fatality.15
-
Long-term Sequelae: Among those who survive severe encephalitis, a significant proportion suffer permanent neurological/cognitive deficits. This makes prevention the only viable strategy for infants who are too young for vaccination or where vaccines are unavailable.
2.2 Ross River Virus (RRV): The Widespread Burden
RRV remains the most common mosquito-borne disease in Australia. In 2024, cases spiked significantly, with reports indicating nearly six times the number of cases compared to the previous year.14 The wet conditions of 2025/26 are expected to sustain high transmission rates throughout the summer and into autumn.
-
Geographic Spread: Early detections have been recorded in the Adelaide Plains (South Australia) and the South West of Western Australia, confirming that the virus is active across the continent.9
-
Symptomatology: While rarely fatal, RRV causes a debilitating illness known as epidemic polyarthritis. Symptoms include swollen and painful joints, fatigue, muscle aches, and a rash.
-
Pediatric Presentation: In children, the presentation can be non-specific and easily misdiagnosed. It often presents as a fever of unknown origin, irritability, and a reluctance to walk or use limbs due to joint pain. The incubation period is 3 to 21 days, making it difficult for parents to link the illness to a specific bite.16
2.3 Murray Valley Encephalitis (MVE) and Kunjin Virus
Like JEV, MVE and Kunjin are flaviviruses capable of causing encephalitis. Kunjin virus was detected in sentinel chickens in Western NSW (Cowra) in late November 2025.17 The confluence of waterbirds (reservoirs) and mosquitoes (vectors) in the Murray-Darling Basin during La Niña years creates a high-risk corridor for these viruses.
Historically, MVE outbreaks occur after heavy rainfall in the catchments of northern Australia flows south into the Murray-Darling system. The current La Niña event replicates the hydrological conditions of the major 1974 and 2011 outbreaks, placing health authorities on high alert.6 There is no vaccine for MVE or Kunjin; avoidance of bites is the sole preventive measure.
2.4 Regional Risk Table (Summer 2025/26)
|
Region |
Primary Viral Threats |
Environmental Driver |
Surveillance Status (Dec 2025) |
|
Victoria (Western/Northern) |
Japanese Encephalitis (JEV) |
Floodwater retention in agricultural zones; Pig farming proximity. |
ACTIVE ALERT: JEV detected in Horsham mosquitoes.8 |
|
New South Wales (Inland) |
Kunjin Virus, JEV, MVE |
Sentinel chicken seroconversion; wet catchment areas in Murray-Darling. |
ACTIVE ALERT: Kunjin detected in Cowra.17 |
|
South Australia (Adelaide Plains) |
Ross River Virus (RRV) |
Coastal saltmarsh inundation and high tides. |
WARNING: Early RRV detection in traps.9 |
|
Western Australia (South West) |
RRV, Barmah Forest Virus |
Spring rains triggering dormant egg hatching in coastal plains. |
WARNING: Virus detected in mosquitoes; no human cases yet.10 |
|
Queensland |
RRV, JEV, Dengue (North) |
Tropical humidity and typical wet season dynamics magnified by La Niña. |
HIGH RISK: Human cases of JEV recorded in 2025.14 |
Part III: Pediatric Vulnerability and the "Mosquito Magnet" Phenomenon
Parents often observe that mosquitoes seem to target their children more aggressively than adults. This is not merely an anecdote; it is rooted in the physiological distinctiveness of infants and toddlers. Understanding why babies are targets is the first step in constructing an effective defense.
3.1 Physiological Attractants in Infants
Mosquitoes utilize a sophisticated array of sensors to locate hosts, detecting chemical, thermal, and visual cues. Infants present a unique profile for these sensors:
-
Thermal Signature: Mosquitoes are highly sensitive to heat differentials. Infants often have higher basal metabolic rates than adults and have a larger surface area relative to their mass. This can result in a higher skin temperature, particularly during sleep or play, creating a distinct thermal plume that mosquitoes can track from a distance.18
-
Carbon Dioxide (CO2) Output: While adults exhale more CO2 in absolute volume, the rapid respiratory rate of infants creates a consistent, pulsed stream of attractant. This CO2 plume acts as the long-range activator for mosquitoes, stimulating them to fly upwind in search of the source.19
-
Olfactory Cues and Microbiome: The human skin microbiome produces volatile organic compounds (VOCs) that either attract or repel mosquitoes. Research suggests that the specific bacterial composition of an individual's skin plays a major role in attractiveness. While this varies by individual, the lack of "repellent" bacteria on the delicate skin of some infants can make them more attractive targets.20
3.2 Skeeter Syndrome: The Pediatric Allergic Response
One of the most distressing aspects of mosquito season for parents is the severity of the reaction on a baby’s skin. A condition known colloquially as "Skeeter Syndrome" is scientifically defined as a large local allergic reaction (LLAR) to mosquito saliva polypeptides.21
3.2.1 The Immunological Mechanism
When a mosquito bites, it injects saliva containing a complex cocktail of anticoagulants (to keep blood flowing), vasodilators, and enzymes. In adults who have been bitten thousands of times, the immune system often develops a tolerance (desensitization). However, infants and young children are immunologically naïve. Their immune system recognizes these saliva proteins as foreign invaders and mounts a vigorous IgE and IgG mediated hypersensitivity response.21
This response results in the release of histamine and leukotrienes, causing intense vasodilation and fluid leakage into the tissues. Because a baby's skin is looser and more delicate than an adult's, the resulting swelling can be dramatic. A bite on the forehead can cause an eye to swell shut; a bite on the hand can make it look like a boxing glove.
3.2.2 Skeeter Syndrome vs. Cellulitis: A Diagnostic Guide
A critical diagnostic challenge for parents is distinguishing between a severe allergic reaction (Skeeter Syndrome) and a secondary bacterial infection (Cellulitis). Misdiagnosis can lead to unnecessary antibiotic use or, conversely, a delay in treating a dangerous infection.
|
Feature |
Skeeter Syndrome (Allergy) |
Cellulitis (Infection) |
|
Onset Timing |
Rapid. Swelling typically appears within hours of the bite and peaks at 24-48 hours.23 |
Delayed. Typically appears days after the bite, often after the skin has been broken by scratching.21 |
|
Visual Appearance |
Large, puffy, red, warm swelling. Can mimic a bruise or hive. Borders may be indistinct.21 |
Red, spreading streak or patch. Skin may appear "pitted" like an orange peel (peau d'orange).24 |
|
Sensation |
Intense Itching (Pruritus) and pain/tenderness.25 |
Pain and Tenderness are dominant; often accompanied by throbbing. |
|
Systemic Signs |
Low-grade fever is possible in very severe cases.21 |
High fever, chills, and swollen lymph nodes are common indicators of systemic infection.24 |
|
Progression |
Swelling usually resolves on its own without antibiotics over 3-7 days. |
The redness spreads continuously over time if untreated. |
Note: In infants, Skeeter Syndrome can cause swelling so severe that it causes immense parental anxiety. If the child is otherwise well (alert, feeding, no high fever), it is likely an allergic reaction. However, any fever in a neonate (<3 months) warrants immediate medical review..23
Part IV: The Repellent Dilemma: Chemical vs. Natural
The choice of repellent for infants is a delicate balance between efficacy (protection from serious disease) and toxicology (safety for the developing organism). Australian health guidelines, supported by international data, provide strict age-stratified recommendations that parents must navigate.
4.1 The Synthetic Standard: DEET and Picaridin
DEET (N,N-diethyl-m-toluamide) has been the global gold standard for mosquito repellency since the 1950s. It works by interfering with the mosquito's olfactory receptors, effectively "blinding" them to the presence of a host.
-
Efficacy: DEET offers the longest duration of protection. A 20-30% concentration can protect for approximately 5-6 hours. It is highly effective against a broad range of vectors, including those carrying JEV and RRV.27
-
Safety Profile: While generally considered safe when used as directed, there are historical concerns regarding neurotoxicity in rare cases of gross overuse or ingestion.
-
Infant Restrictions:
-
< 2 Months: No chemical repellent is recommended. Protection must be physical (clothing, netting).29
-
2 - 12 Months: Repellents with up to 10% DEET or Picaridin are permitted but should be used sparingly. Picaridin is often preferred for children as it is odorless and less oily, though DEET remains the benchmark for high-risk zones.29
-
Application Protocol: Repellent should never be applied to a baby’s hands or near their mouth/eyes to prevent ingestion. It should be washed off once the child returns indoors.30
4.2 The Natural Alternative: Mechanism and Limitations
For parents wary of synthetic chemicals, or for those managing protection in lower-risk environments (e.g., backyard play vs. deep bushwalking), natural repellents are often the preferred choice. However, the category of "natural" requires scrutiny regarding efficacy and reapplication frequency.
4.2.1 Citronella and Essential Oils
Citronella oil (Cymbopogon nardus) is a biopesticide with a non-toxic mode of action.
-
Mechanism: Unlike DEET, which jams receptors, Citronella works primarily by masking human attractants (CO2 and lactic acid). It creates a vapor barrier that confuses the mosquito.
-
The Volatility Problem: The primary limitation of essential oils is volatility—they evaporate quickly. Studies show Citronella efficacy drops significantly after 1-2 hours, with protection rates falling from >90% to <60% rapidly without reapplication.31
-
The Reapplication Imperative: To match the protection profile of DEET, natural repellents must be reapplied more frequently—typically every 2-3 hours. Failure to do so leaves the child vulnerable as the vapor barrier dissipates.32
4.2.2 The PMD vs. OLE Distinction
There is a critical safety distinction to be made between natural Oil of Lemon Eucalyptus and its synthesized or refined active compound, PMD (para-menthane-3,8-diol).
-
PMD Restriction: The CDC and Australian health authorities recommend against using pure PMD products on children under 3 years old. This is due to a lack of safety data on the refined chemical and potential skin irritation.29
-
Essential Oil Safety: Conversely, products containing natural lemon-scented eucalyptus oil (Corymbia citriodora) as part of a lower-concentration blend are often marketed for younger children, provided they do not contain the high-concentrate PMD isolate. Parents must read labels meticulously to distinguish between "PMD" (chemical extract, age 3+) and "Lemon Scented Eucalyptus Essential Oil" (botanical ingredient, often used in younger formulations).29
4.3 Comparative Efficacy Analysis
|
Active Ingredient |
Concentration |
Approx. Protection Time |
Age Suitability (Australia) |
|
DEET |
10% |
~2 Hours |
> 2 Months 29 |
|
DEET |
30% |
~5-6 Hours |
> 2 Months (use caution) 36 |
|
Picaridin |
10% |
~2 Hours |
> 12 Months (SA Health) / > 2 Months (RCH) 29 |
|
Citronella Oil |
Variable (Natural) |
~1-2 Hours (rapid decay) |
Safe for infants (in formulations) 35 |
|
Lemon Eucalyptus Oil |
Natural Blend |
~2 Hours |
> 3 Years for PMD; check label for oil 29 |
Part V: The "Kidsbliss" Approach: Analyzing the Organic Formulation
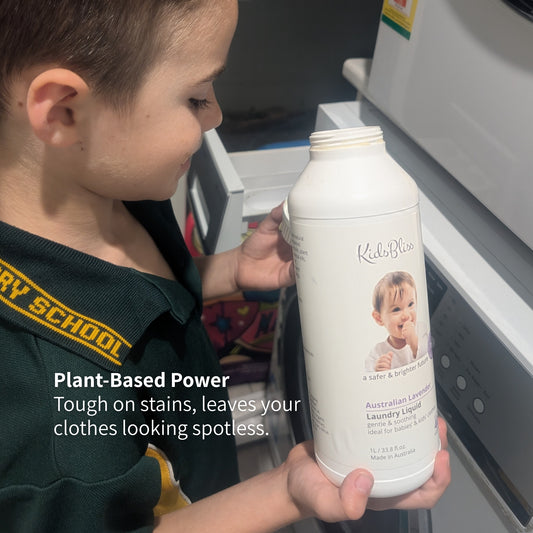
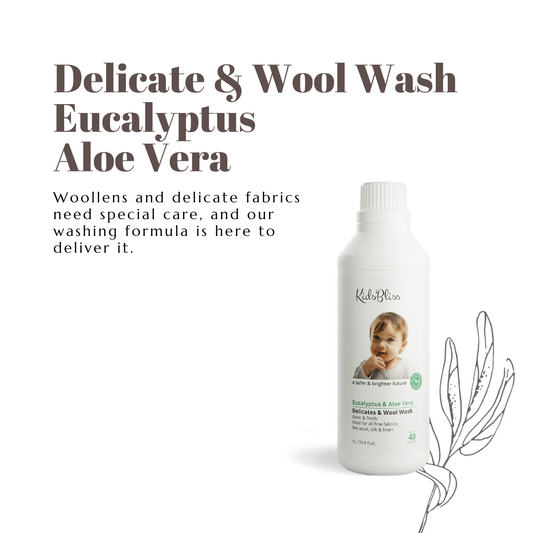
In the context of the 2025 La Niña summer, the Kidsbliss Australian Certified Organic Outdoor Skin Mist presents a case study in balancing safety with natural efficacy. Based on the provided ingredient lists and product specifications, we can analyze its role in a protection strategy for the 2025/26 season.
5.1 Ingredient Profile and Functional Benefits
The formulation relies on a synergistic blend of botanicals rather than a single chemical active. This "stacking" of ingredients aims to broaden the spectrum of repellency while caring for the skin.
-
Organic Citronella Essential Oil: The primary repellent active. As noted, this provides effective short-term deterrence against mosquitoes by masking host odors. Its efficacy is well-documented for short-duration exposure.35
-
Organic Aloe Vera Juice: This is a crucial addition for pediatric skin. Aloe Vera acts as a carrier but also provides a "gentle film" over the skin. Pharmacological studies suggest Aloe has anti-inflammatory and antipruritic (anti-itch) properties. While not a strong repellent on its own, its presence may preemptively soothe the skin and potentially reduce the severity of local reactions (histamine flare) if a bite occurs.37
-
Organic Lemon Scented Eucalyptus Oil: Included for its aromatic profile and synergistic repellent properties. As a natural essential oil component rather than refined PMD, it fits the "natural" profile, though parents of very sensitive infants should always patch test.35
-
Organic Lavender Essential Oil: Lavender contains linalool, which has modest repellent properties, but its primary role here is likely soothing the skin and providing a pleasant, non-chemical aroma that is calming for the child.35
-
Coco Glucoside: A natural surfactant derived from coconut and fruit sugars. It helps mix the essential oils with the water base (emulsification) without the need for harsh synthetic solvents or high levels of alcohol, which can dry out and irritate a baby's developing skin barrier.40
5.2 The "Certified Organic" Standard (ACO)
The product carries the "Australian Certified Organic" (ACO) seal. In the cosmetic industry, where terms like "natural" are often unregulated marketing fluff, this certification provides a rigorous framework of trust.
-
Regulatory Rigor: Under the Australian Certified Organic Standard, products must contain at least 95% certified organic ingredients to carry the bud logo. The remaining ingredients must be naturally produced and strictly restricted (e.g., no GMOs, no synthetic fragrances, no parabens).41
-
Synthetic Prohibition: The standard explicitly prohibits the use of synthetic pesticides or fumigants in the supply chain of the ingredients. For parents concerned about the "cocktail effect" of multiple chemical exposures—especially given the widespread use of agricultural pesticides in the broader environment—this certification provides a verified chain of custody for purity.42
5.3 Usage Protocol for Kidsbliss
To maximize the effectiveness of a natural formulation like Kidsbliss during a high-pressure La Niña season, the following protocol is recommended:
-
Shake Well: Essential oils can separate from the water base over time.
-
Apply Liberally: Natural repellents rely on creating a complete vapor barrier; mosquitoes will find and exploit any missed spots (such as ankles or behind ears).
-
The 2-Hour Rule: Unlike DEET, which persists, this mist should be reapplied every 2 hours, or more frequently if the child is sweating or in high humidity. The "all night long" protection claim should be viewed with caution in high-risk zones; reapplication or complementary netting is safer.44
-
Barrier Method for Infants: For infants under 6 months (or for parents extra cautious about topical applications), spraying the clothing or the pram netting rather than direct skin saturation is a highly effective strategy. This creates a repellent "halo" without direct dermal absorption.36
Part VI: Physical Protection Strategies
While chemical and natural repellents are the second line of defense, physical exclusion remains the primary, safest, and most effective method for protecting babies, particularly those too young for topical applications.
6.1 The Physics of Netting: Mesh Size Matters
Not all mosquito nets are created equal. In Australia, the threat is not just from mosquitoes but also from biting midges (sandflies), which are significantly smaller and can inflict painful, itchy bites that easily penetrate standard netting.
-
Standard Mosquito Mesh: Typically has a mesh size of roughly 1.0mm x 0.9mm. This stops mosquitoes (Aedes/Culex) effectively but allows midges to pass through almost unimpeded.45
-
Midge/Sandfly Mesh: To stop midges, parents require a much tighter weave, typically around 0.6mm x 0.6mm (approx. 600 microns) or a "micromesh" designation. Products like the Outlookbaby Universal Mosquito Net or specific Dreambaby insect netting are designed with this finer gauge in mind.46
-
Airflow vs. Protection Trade-off: The trade-off with tighter mesh is reduced airflow (up to 40% reduction). In a hot Australian summer, this can lead to overheating in prams. Parents should look for "high airflow" midge mesh or ensure the pram is in the shade and potentially use a clip-on pram fan when using fine-gauge netting to maintain air circulation.48
6.2 Chromatic Defense: The Science of Clothing Color
Recent research from the University of Washington has identified that mosquitoes are visually attracted to specific wavelengths of light, overturning the idea that they only hunt by scent.
-
The Red/Orange Signal: Human skin, regardless of pigmentation, emits a long-wavelength signal in the red-orange range. Mosquitoes are highly attracted to this spectrum, especially after they have detected CO2.18
-
High Attractant Colors: Black, Red, Cyan, and Orange. Wearing these colors (or dressing a baby in them) significantly enhances the child's visual profile to the insect. Black also traps heat, increasing the thermal signature.49
-
Repellent Colors: White, Green, Blue, and Purple. Mosquitoes largely ignore these colors in visual tests.
-
Actionable Advice: Dress babies in loose-fitting, light-colored clothing (White/Pale Blue/Pale Green). This serves a dual purpose: it creates a visual "blind spot" for the mosquito and makes it significantly easier for parents to spot a dark insect landing on the child before it can bite.49
6.3 Environmental Modification: The Home Front
Managing the home environment is critical during La Niña to reduce the "source pressure."
-
The 7-Day Cycle: Mosquitoes can complete their life cycle in standing water in as little as 7 days in warm weather. Homeowners must empty bird baths, pot plant saucers, toy buckets, and clear gutters weekly. A single saucer can breed hundreds of mosquitoes.9
-
Screens: Ensure household window screens are intact. A single tear can allow hundreds of insects inside during a humid night. Repairs should be made with midge-grade mesh where possible.51
-
Residual Surface Sprays: For outdoor entertaining areas, applying a residual barrier spray to fences and foliage (where mosquitoes rest during the day) can reduce adult numbers, though this should be kept away from areas where children directly play.
Part VII: Acute Management: When the Bite Happens
Despite best efforts, bites occur. Managing the reaction in infants requires immediate care to prevent the "itch-scratch" cycle which leads to infection.
7.1 Immediate Care Protocol
-
Wash the Site: Immediately clean the bite with soap and water. This removes any lingering saliva on the surface and cleanses bacteria from the mosquito's legs that could cause infection.52
-
Cold Compress: Apply an ice pack (wrapped in a cloth) for 10 seconds. This is the most effective immediate intervention. It constricts blood vessels (limiting the spread of the saliva protein) and numbs the nerve endings to reduce itching.52
-
Topical Relief: A paste of baking soda and water or a soothing aloe vera gel (like the Kidsbliss formulation or pure gel) can reduce itching. Aloe vera has been shown to reduce inflammation and promote healing, making it a valuable addition to the first-aid kit.52
7.2 Pharmacological Intervention (Caution Required)
Parents must be extremely careful with over-the-counter medications for infants.
-
Antihistamines:
-
Sedating (First Generation): Drugs like Promethazine (Phenergan) are contraindicated for children under 2 years (and often under 6) due to risks of respiratory depression, fatal adverse events, and paradoxical agitation.54 Do not use these for sleep or itch in babies.
-
Non-Sedating (Second Generation): Medicines like Cetirizine (Zyrtec) or Loratadine (Claratyne) may be safer for older infants (>6-12 months) but should only be administered under strict medical advice and dosage calculation.56
-
Topical Steroids: A mild 0.5-1% hydrocortisone cream can be used for severe inflammation to reduce the swelling of Skeeter Syndrome, but this should be discussed with a GP before application to an infant's face or extensive body areas.57
7.3 When to See a Doctor
Medical attention should be sought if:
-
The swelling is rapidly spreading or there is red streaking (signs of cellulitis).
-
The child has a fever (especially high fever >38°C).
-
There is swelling of the face, eyes, or lips.
-
The child appears lethargic, is vomiting, or has a stiff neck (potential signs of encephalitis).
Conclusion and Strategic Action Plan
The 2025/26 La Niña summer represents a "perfect storm" for mosquito-borne disease in Australia. The convergence of high rainfall, warm sea surface temperatures, and early viral detections demands a proactive, layered, and intelligent defense strategy.
For parents, the goal is not just to kill mosquitoes, but to create an exclusion zone around the vulnerable infant. This is best achieved through a hierarchy of controls:
-
Avoidance: Limit outdoor exposure during dawn and dusk peak feeding times, especially near wetlands.
-
Exclusion: Use pram nets with midge-grade mesh and dress infants in "mosquito-blind" colors (White/Green/Blue).
-
Repulsion: Utilize safe, natural repellents like the Kidsbliss Certified Organic Skin Mist. Its formulation of Citronella and Aloe Vera offers a safe, non-toxic barrier that protects without the neurotoxic risks associated with heavy chemical use. However, parents must commit to the reapplication discipline—spraying every 2 hours to maintain the vapor barrier.
-
Surveillance: Be vigilant for the signs of Skeeter Syndrome vs. Cellulitis and seek medical attention if a child develops fever, lethargy, or rapid swelling, keeping in mind the incubation periods of JEV and RRV.
By understanding the biology of the threat and the chemistry of the defense, Australian families can safely navigate this wet summer, ensuring that the only thing biting is the fish, not the bugs.
Appendix: Quick Reference Tables
Table A: 2025/26 Viral Threat Watch
|
Virus |
Vector |
Primary Symptom |
Risk Zone (2025) |
|
Japanese Encephalitis (JEV) |
Culex |
Brain swelling, seizure, coma |
VIC, NSW, QLD (Murray-Darling) |
|
Ross River Virus (RRV) |
Aedes/Culex |
Joint pain, fatigue, rash |
National (Coastal/Inland) |
|
Murray Valley Encephalitis |
Culex |
Encephalitis |
Inland WA, NT, NSW |
|
Barmah Forest Virus |
Aedes |
Similar to RRV but milder |
Coastal WA, NSW |
Table B: Repellent Safety Guide for Infants
|
Age Group |
Recommended Product |
Application Method |
|
0 - 2 Months |
None |
Physical barrier only (Clothing, Netting). |
|
2 - 12 Months |
Natural (e.g., Kidsbliss) / Low DEET (<10%) |
Apply to clothing or pram primarily. Patch test skin first. |
|
12+ Months |
Natural / Picaridin / DEET |
Apply to exposed skin. Avoid hands/eyes. |
|
3+ Years |
All Types (inc. PMD/OLE) |
Standard application. |
Table C: "Mosquito-Proofing" Your Baby Checklist
-
[ ] Clothing: Long sleeves, loose fit.
-
[ ] Color: White, Light Blue, Light Green. (Avoid Red, Black, Orange).
-
[ ] Pram: Fitted with "Midge-Grade" mesh (approx. 0.6mm).
-
[ ] Skin: Apply organic repellent (Citronella/Aloe base) every 2 hours.
-
[ ] Home: Verify fly screens are intact; remove standing water weekly.